Anna Lindfors and Heather E. Branigan, University of Aberdeen
ASMR is a sensory-perceptual experience in which specific audio-visual or haptic stimuli reliably trigger electro-static-like ‘brain tingles’ extending peripherally from the back of the scalp. While generally an under-studied phenomenon, research is beginning to identify potential therapeutic benefits of immersing in ASMR-content, supported by anecdotal accounts from active online communities. The present mixed-methods online study aimed to explore the phenomenological aspects of ASMR and its potential therapeutic effects. A total of 224 participants watched ASMR-videos and completed scales measuring ASMR response and affect. Participants then completed four open-ended questions about their ASMR experience and use. In line with our hypotheses, quantitative results suggested that participants who experienced ASMR demonstrated significantly higher positive affect and significantly lower negative affect compared to those who did not (or were unsure about whether they did) experience ASMR. The pleasurability and intensity of ASMR also positively correlated with measures of positive affect, and negatively with measures of negative affect. Thematic analysis identified great phenomenological variability in perceived pleasurability and intensity of ASMR experience among individuals as a super-theme present across themes (Psychological, Physical and Social dimensions). Based on these findings, a multi-dimensional model for characterising ASMR is proposed, providing clear opportunities for future research.
Keywords: ASMR, autonomous sensory meridian response, misophonia, human sensory-perceptual experience, theoretical development grounded in data, multi-dimensional model, social connectedness in ASMR
Imagine seeing a sharp knife cutting into a colourful piece of soap. Once the knife goes through, little pieces of soap fall onto a white surface, which produces an intriguing and oddly satisfying sound. You might start to feel tingles originating from the back of your scalp, down your spine to other areas of your body. The phenomenon you have just imagined is defined in the literature as Autonomous Sensory Meridian Response (ASMR). The tongue-twisting term of ASMR can be described as a sensory-perceptual phenomenon in which specific audio-visual or haptic stimuli reliably trigger electro-static-like tingles that originate at the back of the scalp and extend to peripheral areas of the body (Barratt and Davis, 2015; Barratt et al., 2017). The physical aspect of these ‘tingles’ is considered involuntary, although there seems to be psychological autonomy over the intensity and duration of the response (e.g. choosing to immerse in ASMR-content and experience), which often promotes changes in affect[1] (Poerio et al., 2018). Following anecdotal ASMR-manifestations by self-claimed ‘ASMRtists’ (content creators; e.g. Creative Calm ASMR) and active user-communities, growing research interest is directed towards the origins and implications of this under-studied and even mysterious phenomenon. The focus of the present mixed-methods study is to bring insight into the phenomenological aspects and applications of ASMR.
Commonly reported reasons for use indicate that ASMR-content is used to relax (86–98 per cent), sleep (41–82 per cent), cope with stress (70 per cent) and reduce anxiety (11 per cent) (Barratt and Davis, 2015: 5; Lochte et al., 2018: 302). ASMR often contains ‘person-centric triggers’ in socially intimate content or ‘non-person-centric triggers’ that are more abstract in nature and object-focused (e.g. crisp sounds, repetitive and slow task completions) (Barratt et al., 2017; Fredborg et al., 2018). One of the few studies so far investigating ASMR suggests that both the use and experience of ASMR vary greatly among individuals (McErlean and Banissy, 2018), although some studies suggest that the effect of ASMR is stronger when receiving personal attention and care (Lochte et al., 2018; Smith et al., 2019). Brain-imaging ASMR studies, such as Lochte et al. (2018), have associated activity in the brain during ASMR with brain areas related to social cognition that become active during caring behaviour (e.g. being soothed by a parent). This resembles grooming behaviour in animals (Colonnello et al., 2016) and has been tied to the socially intimate nature of ASMR-content (Barratt et al., 2017; Poerio et al., 2018), suggesting that ASMR could simulate naturally occurring caring behaviour and thus promote neuroprotective aspects of positive social interactions (Colonnello et al., 2016; Lochte et al., 2018; Poerio et al., 2018).
First studies into potential therapeutic implications of ASMR suggest that immersing[2] in ASMR-content can have relaxing and calming effects (Fredborg et al., 2018; Poerio et al., 2018). For instance, immersing in ASMR-content has been shown to provide short-term relief from anxiety (Ditchburn and Bedwell, 2018), stress, depression and chronic pain for up to three hours after viewing content (Barratt and Davis, 2015). Notably, ASMR has been reported to provide relief of symptoms and promote subjective wellbeing even when other therapeutic approaches (such as medical interventions) have been ineffective (Barratt and Davis, 2015). In addition to psychological affect (e.g. feeling calm), effects of ASMR have been observed through physiological affect: ASMR-tingles have led to higher skin conductance and decreased heart rate (Poerio et al., 2018).
At the other end of these pleasure-producing triggers is misophonia – a contrasting sensory-perceptual experience in which common ASMR-triggers such as mouth sounds (e.g. chewing) can produce severe disgust and irritation (Bernstein et al., 2013; Schröder et al., 2013). However, some reports suggest that 49 per cent of those who experience misophonia also experience ASMR (Rouw and Erfanian, 2018). Some suggest that the prevalence of misophonia is even higher in those who experience ASMR (ASMR-experiencers) (McErlean and Banissy, 2018), which has led some to hypothesise that these contrasting sensory experiences could reflect opposite ends of a spectrum (Barratt and Davis, 2015: 13). Additionally, given the heterogeneous nature of the phenomenon, suggestions of defining ASMR on dimensional terms to represent the broad range of individual responses to ASMR-stimuli have begun to emerge in the literature (e.g. Hostler et al., 2019; McErlean and Banissy, 2018; Roberts et al., 2019). Taken together, these empirical findings support the existence and distinction of ASMR as a unique sensory experience that should be further investigated to understand and define its expansive phenomenology.
As ASMR is an under-studied phenomenon, there are several unanswered questions relating to the subject. Given the heterogeneous nature of the phenomenon, variability in anecdotal ASMR experiences (McErlean and Banissy, 2018) and the aforementioned hypothetical suggestions for a spectrum-based view of ASMR (Barratt and Davis, 2015), the existing dichotomous distinction between ASMR-experiencers and non-ASMR-experiencers (those who do not experience ASMR) seems inadequate. To explore the range of individual experiences associated with ASMR, then, a mixed-methods design was deemed as appropriate to gain more in-depth insights into this expansive phenomenon.
The current online study investigates the potential therapeutic implications utilising quantitative and qualitative measures in a sequential explanatory method (Creswell, 2011). Multiple factors are taken into consideration to build and strengthen a systematic foundation for ASMR research. We investigate potential therapeutic implications of immersing in ASMR-videos using measures of affect and ASMR experience. Based on prior findings, we expect to find higher positive affect and lower negative affect among those who experience ASMR compared to those who do not or are unsure of their experience (Hypothesis 1). We also expect to find a relationship between ratings of ASMR (pleasurability/intensity) and affect (Hypothesis 2). Furthermore, we conduct a thematic analysis (Braun and Clarke, 2006) to gain understanding of the phenomenological aspects of ASMR experience and use. Our qualitative analysis is guided by the research question: How do participants describe the experience of immersing in ASMR? Thus, the current study is novel in its use of mixed methods to provide insights into the phenomenology of ASMR.
In total, 231 volunteers participated, of which 9 were excluded due to incomplete consent forms, leaving a sample of 222 (68 males; 1 prefer not to say). The sample consisted of undergraduate students of the University of Aberdeen (UoA) and volunteers from online communities (Mage= 24,95, SD= 8,63). Participants for this online study were recruited through opportunity sampling via social media channels (e.g. Reddit, Facebook, Instagram) and the participant recruitment programme of UoA (SONA) between December 2019 and February 2020. Participants recruited via SONA were compensated 1 SONA credit for their time, whereas participants recruited via social media channels volunteered their time. Due to the exploratory nature of the study and sampling method used, a priori power analysis to calculate an ideal sample size would have been speculative at best and therefore was not conducted.
Ethical approval was obtained from the University of Aberdeen School of Psychology ethics committee, and the study was conducted in accordance with the BPS Code of Human Research Ethics (British Psychological Society, 2014). The online survey was administered using Snap Surveys Webhost. Internal consistency in the present study was measured with Cronbach’s alpha for each questionnaire. After providing informed consent, participants completed the following questionnaires in the order presented:
The multi-affect indicator (Warr et al., 2014)
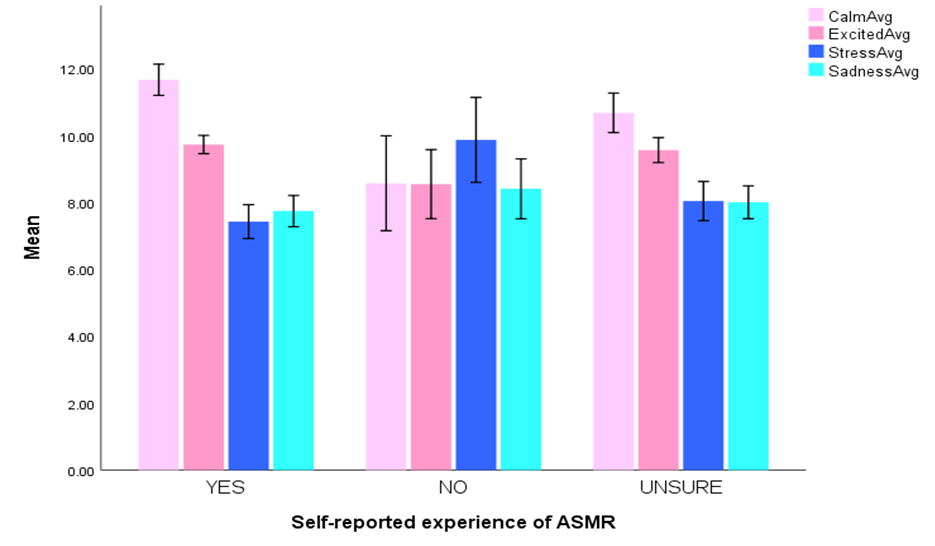
An edited form of the Multi-Affect Indicator (MAI) was administered before (baseline) and after ASMR-videos. Similar to Poerio et al. (2018), we added a measure of social connectedness, given that social connectedness has been proposed to be linked to ASMR in previous literature (e.g. Lochte et al., 2018). Thus, the MAI was used to measure affect and social connectedness. The MAI includes 12 items assessing pleasure and arousal – two dimensions of core affect. Participants were asked to rate their level of affect (‘Please indicate how you feel now compared to before you watched the videos’, e.g. connected with others, excited, dejected; See Appendix A for the full scale) on a Likert scale from 1 (much less) to 7 (much more). The MAI subscale scores were based on four categories of items, with three items describing each particular affect within each category. The four categories were: Calm: Low activation of pleasant affect (calm, relaxed, at ease; α=.94); Excited: High activation of pleasant affect (enthusiastic, joyful, excited; α=.79); Stress: High activation of unpleasant affect (anxious, nervous, tense; α=.91); Sadness: Low activation of unpleasant affect (depressed, dejected, hopeless; α=.88).
The ASMR checklist (Fredborg et al., 2017)
A modified version of the ASMR checklist was included in the study in two parts (before and after immersing in ASMR-videos) to measure participants’ perceived pleasure, intensity and duration of ASMR, ASMR-triggers and use of ASMR. The original version includes 16 ASMR-triggers, but only the ones present in video clips used in the current study were included (i.e. whispering, soft-spoken voice, tapping sounds, scratching sounds, squeezing sounds, soap cutting; see below for description). In the ASMR checklist, intensity and duration of each stimulus were rated on a seven-point Likert scale ranging from ‘0 No tingles’ to ‘6 Most intense ASMR’. An option ‘Unsure’ was offered for individuals who could not identify the onset or duration of the tingles, which was important since the sample was expected to entail both experienced ASMR-users as well as ASMR-novices. In addition, overall pleasurability of ASMR experience was rated on a five-point Likert scale ranging from ‘1 Quite uncomfortable ’ to ‘5 Quite pleasurable’. ASMR-groups in the study were formed based on responses (Yes, No, Unsure) in the ASMR checklist. Following the questions of ASMR-triggers, participants were asked about their use of ASMR-content (e.g. for sleep or to aid relaxing). Participants were also asked to indicate whether they experienced misophonia to distinguish between those sensory phenomena similar to previous literature (Del Campo and Kehle, 2016) (See Appendix A). Internal consistency for the edited version of the ASMR checklist administered in the current study was adequate for the entire scale (α=.74), for intensity ratings (α=.84) and for duration (α=.89).
Video clips
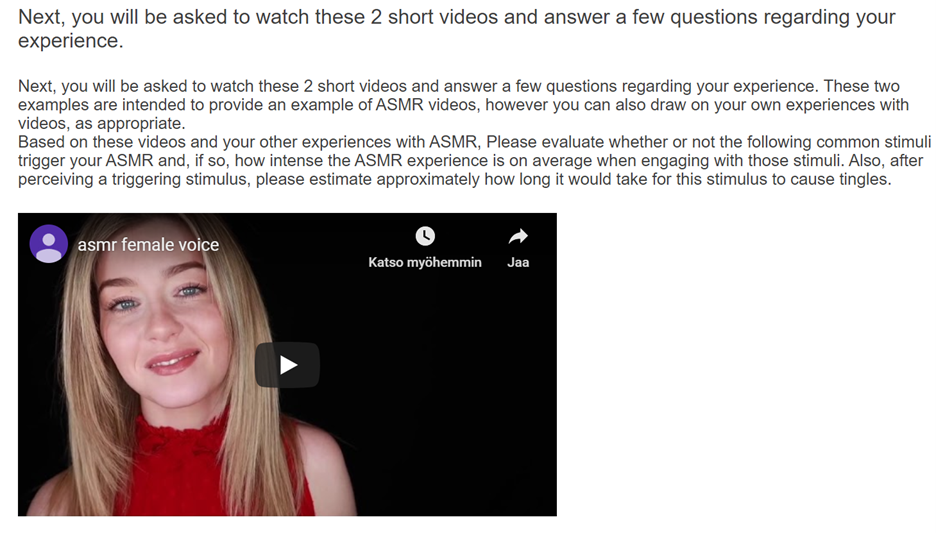
Participants were asked to watch two short ASMR-videos to provide examples of ASMR-eliciting content and common ASMR-triggers. Videos were chosen based on their representability of different ASMR-triggers (Barratt et al., 2017) and popularity (based on number of views) on YouTube (see Appendix B). The original videos sourced from YouTube were edited into two short video clips: non-person-centric (1:40 min) and person-centric (3:00 min) using iMovie v.10.1.13 (Apple, 2019) to provide examples of ASMR-eliciting stimuli. The timeline requirements were enforced in the duration of the videos to prevent participant dropout and loss of data. Video 1 contained ‘person-centric’ triggers (i.e. personal attention) through a woman speaking softly and whispering. A video with a female ‘ASMRtist’ was chosen to represent the majority of ASMR-content being produced by females (Iossifidis, 2017). Video 2 contained various non-person-centric triggers such as scratching, tapping, squeezing and soap cutting. Participants were instructed to wear headphones to fully experience the audio content of the videos. They were also instructed to focus on the intensity and onset of tingles while watching the videos.
Open-ended questions
To explore how participants describe the experience of using ASMR, participants were asked four open-ended questions:
1 Have you seen any of the videos before? If yes, please indicate which one(s) below.
2 Describe the experience of watching an ASMR video.
3 If you use ASMR, why? (e.g. sleep, relax, meditation, etc.)
4 Why do you think you experienced or did not experience ASMR?
This online study employed an exploratory design utilising both quantitative and qualitative measures. The mixed-methods design of the present study was conducted in a sequential explanatory method, meaning that the qualitative measures were employed to support quantitative findings (Creswell, 2011). Between-subjects and correlational analyses were conducted to analyse the quantitative data, and a thematic analysis was performed to explore the qualitative dataset. We chose a bivariate correlation to investigate and represent the heterogeneous and complex nature of ASMR. This method was chosen based on previous findings (e.g. Poerio et al. 2018).
Thematic analysis
A thematic analysis (TA) was conducted to explore the qualitative research question. TA was chosen as it is not attached to any pre-existing theoretical framework. Therefore, it is a flexible tool that can be used from several different methodological standpoints, which makes it useful for mixed-method designs (Creswell, 2011). The TA was conducted via the realist method as reported experiences of participants were considered to represent their reality (i.e. true experience). Moreover, we drew on insights from grounded theory, which allowed a systematic yet flexible manner for constructing theory grounded in the data through substantive analysis of the dataset (Strauss and Corbin, 1994). This method is often utilised when little is known about the phenomenon (Chun Tie et al., 2019), which makes it appropriate for the current study.
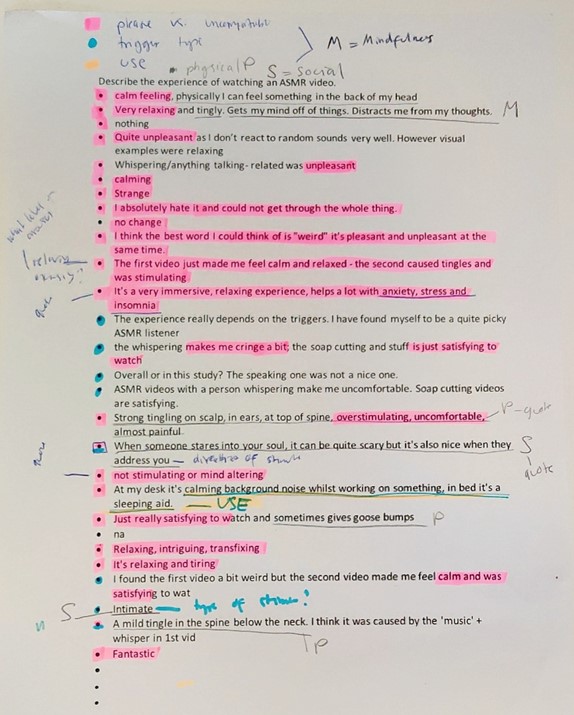
Qualitative data from four open-ended questions were analysed according to Braun and Clarke’s guidelines (2006). The steps were as follows: (1) We[3] familiarised ourselves with the data by reading and re-reading the data multiple times throughout several weeks and noting down initial ideas and preliminary codes. (2) Initial codes were created manually based on identified ideas. Each code was assigned a colour, which were used to systematically highlight and collate data relevant to each code across the entire dataset. (3) All data relevant was collated under each code under potential themes and sub-themes. (4) Potential themes were revisited and contrasted to collated code extracts (Level 1), and thematic maps of the analysis were created (Level 2) (see Appendix C). (5) Themes were defined and discussed in research group meetings, after which themes were refined. After following these steps, themes were revisited to ensure coherence with other themes and in relation to the whole dataset. (6) Extracts were selected from the dataset to provide illustration of the themes identified during the analysis. During the selection, we related back to the analysis conducted in relation to the research question and study aim to ensure that the extracts chosen were representative. Existing literature was revisited after TA to connect identified constructs with current knowledge.
Multiple data analyses were conducted to explore the phenomenological aspects of ASMR and its potential therapeutic implications. The order of the results presented in this section follows the order of the hypotheses and research question of the present study. Means and Standard Deviations of scales are presented in Table 1.
|
|
ASMR Yes (n= 106) |
ASMR No (n= 36, n_calm= 37) |
ASMR Unsure (n= 79)
|
|
Calm
|
11.67 (2.43) |
8.41 (4.26) |
10.68 (3.09) |
|
Excited
|
9.73 (1.41) |
8.55 (3.05) |
9.57 (1.89) |
|
Stress
|
7.43 (2.62) |
9.87 (3.75) |
8.04 (2.95) |
|
Sadness |
7.74 (2.42) |
8.41 (2.65)
|
8.00 (2.19) |
|
Connectedness |
4.21 (.86) |
4.06 (1.31) |
4.09 (.79) |
|
|
|
|
Notes: n refers to sample size. Participants were allocated into self-assigned ASMR-groups (Yes, No, Unsure) based on their responses in the ASMR checklist.
To investigate our hypotheses concerning the therapeutic implications of ASMR, we conducted a correlation between ASMR dimensions (Pleasure and Intensity) and affect (MAI), as well as one-way ANOVAs to compare the differences in affect between ASMR-groups.
ASMR pleasurability and intensity
We explored the relationship between ASMR-pleasure (ASMR-(P)) and ASMR-intensity (ASMR-(I)) (or, together, (ASMR-P/I)) ratings and affect measures. As Table 2 shows, multiple significant correlations were found. These findings suggest that higher reported ASMR-(P/I) correlates with higher positive affect (Calm and Excited) and lower negative affect (Stress and Sadness) and lower ASMR-(P/I) ratings with higher negative affect (Stress and Sadness) and lower positive affect (Calm and Excited). Social connectedness was positively correlated with ASMR-I as well as positive affect, and negatively correlated with negative affect. There was no significant correlation with ASMR-P and social connectedness. The strengths of the correlations are presented based on criteria outlined by Evans (1996): very weak (.00–.19); weak (.20–.39); moderate (.40–.59).
| Calm | Sadness | Stress | Excited | Connectedness | ASMR-P | ASMR-I | ||
| Calm | 1 | -.44*** | -.77*** | .65** | .357** | .59*** | .33*** | |
| N | 222 | 221 | 221 | 221 | 222 | 218 | 221 | |
| Sadness | 1 | 64*** | -.31*** | -.338** | -.23*** | -.21** | ||
| N | 221 | 221 | 221 | 221 | 217 | 221 | ||
| Stress | 1 | -.46*** | -.249** | -.50*** | -.25*** | |||
| N | 221 | 221 | 221 | 217 | 221 | |||
| Excited | 1 | .621** | .37*** | .25*** | ||||
| N | 221 | 221 | 217 | 221 | ||||
| Connectedness | 1 | .112 | .189** | |||||
| 221 | 217 | 221 | ||||||
| ASMR-P | 1 | .32*** | ||||||
| N | 218 | 217 | ||||||
| ASMR-I | 1 | |||||||
| N | 221 |
Positive affect
A one-way ANOVA was conducted to explore differences in Calm-subscale scores (from the Multi-Affect Inventory) between self-assigned ASMR-groups signifying the experience of ASMR (Yes, No, Unsure). As Figure 1 shows, there was a significant difference between groups (F(2219)= 17.686, p=.001). Post hoc analyses (Bonferroni correction) revealed that the Yes-group scored significantly higher in the Calm-subscale compared to the No-group (p<.001). The No-group also scored significantly lower than the Unsure-group (p<.001). The Yes-group scored higher in Calm-subscale than the Unsure-group, but the difference was not statistically significant, although approaching significance(p=.072). As Figure 1 shows, there was a significant difference between ASMR-groups in the Excited-subscale (F(2218)= 5.631, p=.004). Post hoc analyses (Bonferroni) revealed that the Yes-group scored significantly higher in the Excited-subscale compared to the No-group (p=.003). The No-group also scored significantly lower in excitement than the Unsure-group (p=.02). There was no statistically significant difference in levels of social connectedness among ASMR-groups.
Negative affect
To explore differences between groups in negative affect of ASMR, a one-way ANOVA was conducted. As Figure 1 shows, we found a significant difference between groups (F(2218)= 9.993, p<.001). Post hoc analyses (Bonferroni) revealed higher reported stress in the No-group compared to the Yes-group (p<.001) and the Unsure-group (p=.005). There was no significant difference between groups in sadness-ratings.
Thematic analysis
A TA was conducted on the full qualitative dataset from the four open-ended survey questions. As detailed below, ‘pleasure versus intensity’ was identified as a super-theme that was prominent across all of the themes presented. Under the broad ‘super-theme’, three themes were identified:
1 Psychological dimension, defined as changes in psychological state resulting from immersing in ASMR-content (i.e. psychological affect)
2 Physical dimension, defined as the extent of ‘tingles’ (i.e. physiological affect)
3 Social dimension, describing perceived interpersonal intimacy of ASMR (i.e. social affect).
An outline of the main themes and sub-themes is presented in Table 3, with example extracts from the full TA provided in Appendix C.
‘Pleasure versus intensity’ super-theme
While conducting the TA, a great division of responses at the opposite ends of both of ASMR-pleasure and -intensity spectrums were identified. That is, a key finding in our analysis was the clear variability in participants’ descriptions of both the intensity and the pleasurability of ASMR. Thus, while participants described the experience of ASMR in Psychological, Physical and Social dimensions, ‘pleasure versus intensity’ was identified as a super-theme that was prominent across all of the themes presented. The presence of this super-theme is marked with * within themes in Table 3.
| Themes | Sub-themes | Example | |
| Psychological dimension | 1 | ‘It’s a very immersive, relaxing experience, helps a lot with anxiety, stress and insomnia.’* | |
| 2 | ‘uncomfortable: It’s like a scratching chalkboard sensation, just without direct pain to my ears.’* | ||
| 3 | ‘I think the best word I could think of is “weird”; it’s pleasant and unpleasant at the same time.’* | ||
| 4 | ‘Relaxing/concentrating while doing other computer tasks, headache relief, help with anxiety.’ | ||
| Misophonia | 5 | ‘I don’t think it’s possible to experience an ASMR response because my misophonia gets triggered.’ | |
| 6 | ‘I’m autistic + misophonia – ASMR things help me stim + cope with other distressing sounds.’ | ||
| Physical dimension | 7 | ‘Mainly for relaxation, but it’s very important that I experience “the tingles” and goosebumps.’* | |
| 8 | ‘I cannot find myself getting tingles, however listening to ASMR can help me calm down.’* | ||
| 9 | ‘It is relaxing and cathartic to experience “tingles”. It’s like scratching an itch.’* | ||
| 10 | ‘Strong tingling on scalp, in ears, at top of spine, overstimulating, uncomfortable, almost painful.’* | ||
| 11 | ‘Mildly unnerving; however, I had the asmr response which made it a lot more enjoyable.’* | ||
| 12 | ‘As if there’s something vibrating in my chest and warmly spreading out (sorta [sic] mindfulness?)’ | ||
| Social dimension | Intimacy | 13 | ‘Makes you feel less alone, gives a calming presence’.* |
| 14 | ‘I feel like someone is interfering with my personal space and being to close to me in general.’* | ||
| 15 | When someone stares into your soul, it can be quite scary but it’s also nice when they address you.’* | ||
| Connectedness | 16 | ‘The voices feel very close up and provide a human connection I otherwise don’t have.’ | |
| 17 | ‘I expect it is in our nature to be calmed by sounds reminiscent of a mother calming her child.’ | ||
| 18 | ‘I have problems falling asleep alone, so especially personal attention ASMR helps me sleep.’ |
Psychological dimension
In the psychological dimension, descriptions of responses to ASMR-videos ranged from extreme intense psychological pleasure (Example 1*) to an extremely intense unpleasurable experience (Example 2*), leaving the rest of participants somewhere in between (Example 3*). As shown in Table 3, misophonia was identified as a sub-theme of the psychological dimension. We found misophonia to be prominent in the dataset, as indicated through either direct descriptions of the term ‘misophonia’ or stark descriptions of psychological discomfort. Some participants appeared to perceive misophonia and ASMR to exclude each other (Example 5), while others reported seeking aid to distressing sounds from ASMR (Example 6). It was interpreted that these constructs provided further insight into a broad range in perceived pleasurability and intensity of responses to ASMR-content.
Physical dimension
The physical dimension related to an experience of ‘tingles’. This physical experience was described in relation to psychological benefits (Example 7*), although some participants reported experiencing psychological benefits without inducing tingles (Example 8*). This suggests that, while often co-occurring, the physical and psychological dimensions can also be considered as being separate. Similar to the psychological dimension, descriptions in the physical dimension varied in the pleasurability and intensity of the physical ‘tingling’ from extreme pleasurability and intensity (Example 9*) to extreme unpleasurable and intense experience (Example 10*), leaving some participants somewhere in between (Examples 11* and 12*).
Social dimension
Analysis of the data suggests that responses to ASMR-content extend beyond the individual’s internal physical or psychological state – to a sense of connectedness and intimacy with others. Some responses suggested a variability in the pleasurability and intensity of perceived intimacy of ASMR experience, ranging from pleasurable associations with social intimacy (Example 13*) to intense unpleasurable experiences (Example 14*). Some participants appeared to have mixed feelings about the pleasurability and intensity of the social intimacy in ASMR-content (Example 15*). The socially intimate nature of ASMR-stimuli promoting feelings of social connectedness was also interpreted from the data (Example 16). The potential of ASMR-stimuli in simulating parental caring behaviour was described (Example 17) and social aspects of ASMR were also identified as a reported purpose for using ASMR (Example 18).
The aim of this mixed-methods study was to provide insights into the phenomenological aspects of ASMR and its potential therapeutic implications. Given the explorative nature of the study, multiple analyses were conducted to gain insight into the phenomenon. Hypothesis 1 was supported since there were significant differences in positive and negative affect between participants who reported experiencing ASMR and those who did not. Hypothesis 2 was also supported, as we found significant correlations between affect and ASMR (Pleasure/Intensity). Moreover, through TA of open-ended responses, we also aimed to gather more in-depth insights from individuals in the phenomenology of ASMR. Our identified themes provided insights into the phenomenological aspects of this expansive phenomenon, suggesting that responses to ASMR-videos extend beyond the level of ‘tingles’ elicited – with participants describing distinct experiences of intensity and pleasurability in physical, psychological and social dimensions associated with ASMR.
Our findings, in line with prior studies (e.g. Poerio et al., 2018), suggest that participants who experience ASMR reported significantly higher positive affect in both Calm- and Excited-subscales compared with non-ASMR-experiencers, with those unsure of whether they experience ASMR scoring in between (significantly lower than ASMR-experiencers and higher than non-ASMR-experiencers). When it comes to negative affect, the situation was reversed, as non-ASMR-experiencers showed significantly higher stress than ASMR-experiencers and the Unsure-group. These results suggest that reported physiological experience of ASMR could impact psychological affect following from immersing in ASMR-content. This observation was supported by our correlational findings: As shown in Table 2, there were significant positive correlations (weak/moderate) with both ASMR pleasurability and intensity, and positive affect as well as significant negative correlations (weak/moderate) with ASMR-(P/I) and negative affect. Additionally, the positive relationship between deactivating (Calm) and activating (Excited) sub-scales of positive affect reflects the emotionally complex and heterogeneous nature of ASMR (Poerio et al., 2018). Together, these findings suggest that not only the experience of ASMR but also perceived pleasurability and intensity of that experience could impact psychological affect when immersing in ASMR-content. When considering the limitations of the present study, it is to be noted that in the ASMR checklist, participants were advised to focus on the onset and intensity of tingles, which could present a potential for expectancy effects for participants regarding their response to ASMR-content (Cash et al., 2018). In future studies, adding control stimulus could be beneficial to help control for expectancy effects.
In relation to the phenomenology of ASMR, it was clear that participants described different responses to ASMR-content, both in our quantitative analyses and from our qualitative analysis. That is, through TA, we identified a great variability in the pleasurability and intensity of ASMR, as some participants appeared to perceive ASMR as an extremely intense and pleasurable experience, whereas some reported having an extremely intense yet very unpleasurable experience. Some reported having a mild, yet pleasurable experience, and others reported low intensity as unpleasurable (see Table 3). These interpretations are consistent with a prior mixed-methods study that also identified a broad range of individual experiences through content analysis (Roberts et al., 2019).
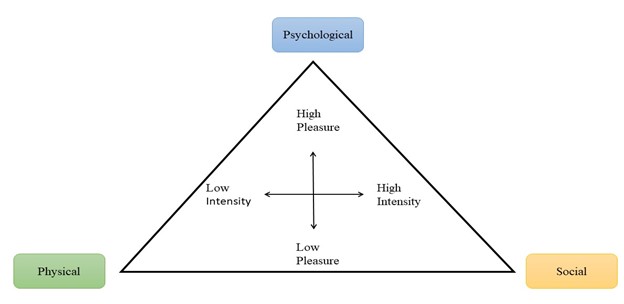
The interpreted variability in individual phenomenological experience both in Pleasure and Intensity of ASMR was identified as a super-theme in our analysis, suggesting that instead of a dichotomous uni-dimensional distinction between ASMR-experiencers and non-ASMR-experiencers, a multi-dimensional view could better represent the broad range of responses. These findings, therefore, led us to develop a new model of ASMR, which uniquely captures the clear spectrums of ASMR-pleasure and ASMR-intensity (see Figure 2). As shown in our model, these (P/I)-spectrums were present across the three dimensions of wellbeing: Psychological, Physical and Social. These dimensions were characterised as distinct yet interconnected. That is, the perceived intensity and pleasurability of the psychological affect could be associated with intensity and pleasurability of physiological experience, but not necessarily – which was apparent in individual reports of the current study (see Table 3). The presence of misophonia and variability among misophonia-experiencers in the TA not only provided support for prior speculations of a spectrum-based view of ASMR (Barratt and Davis, 2015; McErlean and Banissy, 2018), but also in the multi-dimensional intensity–pleasure spectrums highlighted in the current study.
One particularly novel finding of the current research is the addition of a social dimension of ASMR. Indeed, while the role of social intimacy in the hypothesised therapeutic associations of ASMR has been speculated in the literature, it has yet to be integrated with other dimensions in ASMR research. The association of social connectedness with affect and intensity of reported ASMR experience in the present study supports prior findings of the social aspects of ASMR (e.g. Lochte et al., 2018). Furthermore, drawing from reported experiences of social intimacy in the current study, our multi-dimensional model takes into account the perceived pleasurability and intensity of social intimacy in ASMR-content. The aforementioned potential simulation of natural caring behaviour of ASMR-content could ultimately be considered a motivating factor for immersing in the experience to relieve stress, depression, anxiety and pain (Barratt and Davis, 2015; Ditchburn and Bedwell, 2018; Garro, 2017; Turtiainen, 2019). In the future, therefore, incorporating potential therapeutic benefits of social affect (e.g. social connectedness) with psychological and physiological affect in ASMR research could provide insight into the foundation of the phenomenon and assist in creating therapeutic applications of ASMR. Further insights into the social dimension and potential therapeutics implications of ASMR could especially benefit in understanding individual experiences in which physiological ‘tingles’ are not reported, but changes in psychological affect are perceived (See Table 3) – especially since no significant difference was observed in reported connectedness between ASMR-groups (Yes, No, Unsure). Additionally, investigating the role of various ASMR-triggers in mediating social connectedness could provide further insight into ASMR-content and its therapeutic applications.
While this multi-dimensional conceptualisation of ASMR is novel considering the predominantly dichotomised uni-dimensional definition (based on physiological response) in the literature (e.g. Poerio et al., 2018; Smith et al., 2019), our model is consistent with multi-dimensional approaches measuring other affective states. For example, in the Valence–Arousal model (Posner et al., 2005; Russell, 1980), dimensions of emotion are measured through the Valence-continuum (pleasant–unpleasant) and the Arousal-continuum (low–high intensity), and this has been applied to measure the emotion of awe (e.g. Chirico et al., 2017; Stern, 2017). Since ASMR is associated with changes in affect, support for a multi-dimensional categorisation of ASMR also stems from the biopsychosocial model of health (Engel, 1977) that defines wellbeing through interaction of psychological, social and biological processes (Suls and Rothman, 2004).
In relation to ASMR, some ASMR-pioneers have begun to suggest a more dimensional conceptualisation of the phenomenon that would take into consideration the a) degree of intensity varying from mild to extreme, b) extent and location of tingles and c) degree of emotional response (affect) (Hostler et al., 2019). Furthermore, a newly developed scale for ASMR (ASMR-15) has a dimensional approach measuring altered state of consciousness, relaxation, affect and sensation (Roberts, 2019). Therefore, our multi-dimensional model provides a basis for understanding the complexity of the ASMR experience that is not only grounded in the data, but also develops insights from wider literature in this ever-expanding field. Applying this multi-dimensional model both in quantitative scale development as well as multi-modal ASMR research could allow us to better understand and characterise this under-studied phenomenon and, in addition, bring more insight into the full spectrum of human sensory-perceptual experiences and their relationship with wellbeing.
In conclusion, the present mixed-methods study provided insights into the phenomenological aspects of ASMR. Our results suggest that perceived pleasurability and intensity of ASMR are associated with psychological affect that often results from immersing in ASMR. Moreover, our analysis of participants’ descriptions of their ASMR-immersion clearly highlighted a need to reconceptualise ASMR. To this end, our multi-dimensional model of ASMR represents the individual phenomenological variability in perceived pleasurability and intensity of ASMR across Psychological, Physical and Social dimensions of wellbeing. We propose that, going forwards, this model can be applied to ASMR research to provide a basis to more accurately assess the multi-modal complexity of this expansive phenomenon and great variability of individual experiences across identified dimensions.
The authors would like to give special thanks to Ms Laura Zabala for contributing to research group discussions and data collection.
We would also like to take this opportunity to thank Dr Giulia Poerio, Dr Helge Gillmeister and Dr Caroline Barratt for expertise advice and discussions around ASMR.
Last but not least, we want to thank the University of Aberdeen for facilitating our research and Dr Bernhard Scheliga for his expertise assistance in setting up the survey.
Figure 1: Summary of means under each subscale of MAI based on ASMR experience.
Figure 2: Multi-dimensional model of ASMR.
Figure 3: Instructions given to participants before watching ASMR-eliciting videos and screenshot of the first video that contained interpersonal ASMR-triggers.
Figure 4: An example of Stage 2 of the thematic analysis. Initial codes were assigned a colour/symbol that were systematically used to collate data points under each code.
Table 1: Mean Multi-Affect Indicator (MAI) scores.
Table 2: Correlations between Multi-Affect Indicator sub-scales and ASMR-pleasure dimension of ASMR checklist.
Table 3: Summary of the main themes and sub-themes under each theme with illustrative quotes.
The multi-affect indicator (Warr, Bindl, Parker and Inceoglu, 2014)
Please indicate how you feel at the moment using this scale.
Little Neutral Much
1 2 3 4 5 6 7
CIRCLE one
|
connected with others |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
joyful |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
tense |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
relaxed |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
dejected |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
hopeless |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
enthusiastic |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
anxious |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
calm |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
depressed |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
excited |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
at ease |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
|
nervous |
1 |
2 |
3 |
4 |
5 |
6 |
7 |
The ASMR checklist (Modified for the purpose of this study: shorter than original) (Fredborg et al., 2017)
Are you familiar with ASMR? (YES, NO)
Do you experience ASMR response? (YES, NO, UNSURE)
Do you use videos or audio files designed to elicit ASMR response? (YES, NO)
How often do you use ASMR-videos or audio files to help you go to sleep? (Never, Less than Once a Month, 2–3 times a Month, 2–3 times a Week, Daily)
How often do you use ASMR-videos of audio files to help you relax (but not sleep)? (Never, Less than Once a Month, 2–3 times a Month, 2–3 times a Week, Daily)
Misophonia is a strong negative emotional trigger to certain sounds. Triggers for misophonia typically include non-verbal sounds made by the mouth, such as chewing and crunching. Do you experience misophonia? (YES, NO, UNSURE)
Next, you will be asked to watch these 2 short videos and answer a few questions regarding your experience. These two examples are intended to provide an example of ASMR-videos, however you can also draw on your own experiences with videos, as appropriate.
Based on these videos and your other experiences with ASMR, Please evaluate whether or not the following common stimuli trigger your ASMR and, if so, how intense the ASMR experience is on average when engaging with those stimuli. Also, after perceiving a triggering stimulus, please estimate approximately how long it would take for this stimulus to cause tingles.
Intensity scale (higher numbers represent increasing intensity)
|
Stimulus |
Intensity (please circle the appropriate number according to the scale above or select ‘Unknown’) |
How many seconds after its onset do you feel tingles? (please circle one or select ‘Unknown’) |
|
Whispering |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
|
Soft-spoken voice |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
|
Tapping sounds |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
|
Scratching sounds |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
|
Squeezing sounds |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
|
Soap cutting |
0 1 2 3 4 5 6 Unknown |
0–10 31–40 |
Questions about ASMR
Are your experiences more intense when the stimulation is directed towards you (e.g. someone whispering to you)?
Y / N / Unsure
Is your ASMR experience more intense when you observe someone performing an action to/for themselves (e.g. applying their own makeup) rather than when you observe someone acting upon another person (e.g. applying makeup to someone else)?
Y / N / Unsure
Have you ever experienced ‘chills’ from beautiful music?
Y / N / Cannot Recall
If so, does the ASMR feeling differ getting chills from beautiful music?
Y / N / Cannot Recall
On average, how pleasurable is an ASMR experience?
a) Quite Uncomfortable
b) Mildly Uncomfortable
c) Neutral
d) Mildly pleasurable
e) Quite pleasurable
What is the earliest age you can recall having an ASMR experience? (For example, if you remember first having an ASMR experience at the age of four, please choose ‘4’). In this question, a ‘first ASMR experience’ refers to the first time that you noticed you were experiencing ASMR-related tingles, even if at the time you did not know what they were called. If you aren’t sure, make your best guess.
Ad hoc qualitative questionnaire
Finally, we are interested in hearing your thoughts about the experiment in more depth. Please reflect on your emotions and thoughts during the experiment when you answer the following questions.
1. Have you seen any of the videos before? If yes, please indicate which one(s) below.
2. Describe the experience of watching an ASMR video.
3. If you use ASMR, why? (e.g. Sleep, relax, meditation, etc.)
4. Why do you think you experienced, or did not experience ASMR?
Edited videos presented in the study:
ASMR female voice:
https://www.youtube.com/watch?v=4Ea7g8sixuY
ASMR mix:
https://www.youtube.com/watch?v=x-VRnYg9ZBk
[1] Affect is a construct (e.g. psychological) that varies along continuums in three dimensions: Arousal, Valence and Motivation (Harmon-Jones et al., 2013).
[2] The verb ‘immerse’ was used in the present study to describe the act of intentionally exposing oneself to ASMR-eliciting stimuli (e.g. ASMR video) to represent the multi-sensory (visual, auditory, haptic) nature of the phenomenon.
[3] The themes presented in the present study are based on analysis led by the main researcher in this study (the first author). As detailed, in (5), codes and themes were discussed at length among the co-authors, with additional refinement through discussion with an individual external to this research study.
Apple (2019), iMovie (10.1.13), [software], accessed 16 November 2019
Barratt, E. L. and N. J. Davis (2015), ‘Autonomous sensory meridian response (ASMR): A flow-like mental state’, PeerJ, 3, e851. 1–17
Barratt, E. L., C. Spence and N. J. Davis (2017), ‘Sensory determinants of the autonomous sensory meridian response (ASMR): Understanding the triggers’, PeerJ, 5, e3846
Bernstein, R. E., K. L. Angell and C. M. Dehle (2013), ‘A brief course of cognitive behavioural therapy for the treatment of misophonia: A case example’, Cognitive Behaviour Therapist, 6
Braun, V. and V. Clarke (2006), ‘Using thematic analysis in psychology’, Qualitative Research in Psychology, 3 (2), 77–101
British Psychological Society (2014), Code of Human Research Ethics. Leicester: British Psychological Society
Cash, D. K., L. L. Heisick, and M. H. Papesh (2018), Expectancy effects in the autonomous sensory meridian response. PeerJ 6, e5229, doi 10.7717/peerj.5229
Chirico, A., P. Cipresso, D. B. Yaden, F. Biassoni, G. Riva and A. Gaggioli (2017), ‘Effectiveness of immersive videos in inducing awe: An experimental study’, Scientific Reports, 7 (1), 1–11
Chun Tie, Y., Birks, M., & Francis, K. (2019), Grounded theory research: A design framework for novice researchers. SAGE Open Medicine, 7, 205031211882292.
Colonnello, V., N. Petrocchi, M. Farinelli and C. Ottaviani (2016), ‘Positive social interactions in a lifespan perspective with a focus on opioidergic and oxytocinergic systems: Implications for neuroprotection’, Current Neuropharmacology, 15 (4), 543–61
Creswell, J. W. (2011), ‘Controversies in mixed methods research’, in Denzin, N. K. and Y. S. Lincoln, (eds) The SAGE Handbook of Qualitative Research, 4th edn, Los Angeles: SAGE Publications, Inc., pp. 269–82
Del Campo, M. A., & Kehle, T. J. (2016), Autonomous sensory meridian response (ASMR) and frisson: Mindfully induced sensory phenomena that promote happiness. International Journal of School and Educational Psychology, 4(2), 99–105.
Ditchburn, T. A. and S. A. Bedwell (2018), ‘Autonomous sensory meridian response: An ineffective long-term therapeutic intervention’. PsyPAG (110), 19-24.
Engel, G. L. (1977), ‘The need for a new medical model: a challenge for biomedicine’, Science, 196 (4286), 129–36
Evans, J. D. (1996), Straightforward Statistics for the Behavioral Sciences. Pacific Grove: Thomson Brooks/Cole Publishing Co.
Fredborg, B., J. Clark and S. D. Smith (2017), ‘An examination of personality traits associated with autonomous sensory meridian response (ASMR)’, Frontiers in Psychology, 8, 247
Fredborg, B., J. Clark and S. D. Smith (2018), ‘Mindfulness and autonomous sensory meridian response (ASMR)’, PeerJ, 6, e5414
Garro, D. (2017), ‘Autonomous meridian sensory response – from internet subculture to audiovisual therapy’, in Proceedings of the Electronic Visualisation and the Art Conference (EVA London 2017), 2017, p.395-402
Harmon-Jones, E., P. A. Gable and T. F. Price (2013), ‘Does negative affect always narrow and positive affect always broaden the mind? Considering the influence of motivational intensity on cognitive scope’, Current Directions in Psychological Science, 22(4), 301–07
Hostler, T. J., G. L. Poerio and E. Blakey (2019), ‘Still more than a feeling: Commentary on Cash et al., “expectancy effects in the autonomous sensory meridian response” and recommendations for measurement in future ASMR research’, Multisensory Research, 32 (6), 521–31
Iossifidis, M. J. M. (2017), ‘ASMR and the “reassuring female voice” in the sound art practice of Claire Tolan’, Feminist Media Studies, 17 (1), 112–15
Lochte, B. C., S. A. Guillory, C. A. H. Richard and W. M. Kelley (2018), ‘An fMRI investigation of the neural correlates underlying the autonomous sensory meridian response (ASMR)’, BioImpacts, 8 (4), 295–304
McErlean, A. B. J. and M. J. Banissy (2018) ‘Increased misophonia in self-reported autonomous sensory meridian response’, PeerJ, 6, e5351
Poerio, G. L., E. Blakey, T. J. Hostler and T. Veltri (2018), ‘More than a feeling: Autonomous sensory meridian response (ASMR) is characterized by reliable changes in affect and physiology’, PLOS ONE, 13 (6), e0196645
Posner, J., J. A. Russell and B. S. Peterson (2005), ‘The circumplex model of affect: an integrative approach to affective neuroscience, cognitive development, and psychopathology’, Development and Psychopathology, 17 (3), 715–34
Roberts, N. (2019), ‘Autonomous sensory meridian response: induction, personality, and consciousness’, unpublished PhD thesis, Macquarie University
Roberts, N., A. Beath, and S. Boag (2019), ‘Autonomous sensory meridian response: scale development and personality correlates’, Psychology of Consciousness: Theory Research, and Practice, 6 (1), 22–39
Rouw, R. and M. Erfanian (2018), ‘A large-scale study of misophonia’, Journal of Clinical Psychology, 74 (3), 453–79
Russell, J. A. (1980), ‘A circumplex model of affect’, Journal of Personality and Social Psychology, 39 (6),1161–78
Schröder, A., N. Vulink and D. Denys (2013), ‘Misophonia: Diagnostic criteria for a new psychiatric disorder’, PLoS ONE, 8 (1), e54706
Smith, S. D., B. K. Fredborg and J. Kornelsen (2019), ‘A functional magnetic resonance imaging investigation of the autonomous sensory meridian response’, PeerJ, 7, e7122
Stern, W. (2017), ‘Elicitors and effects of an awe experience’, unpublished Master's thesis, University of Oklahoma, 8–83
Strauss, A., & Corbin, J. (1994), Grounded theory methodology: An overview. In N. K. Denzin & Y. S. Lincoln (Eds.), Handbook of qualitative research Sage Publications, Inc., 273–85
Suls, J. and A. Rothman (2004), ‘Evolution of the biopsychosocial model: prospects and challenges for health psychology’, Health Psychology, 119–25
Turtiainen, R. (2019), ’Leikitäänkö kampaajaa? Digitaalinen koskettaminen ASMR-roolileikkivideoissa. [Shall we play hairdresser? Digital touching in ASMR-roleplay.]’ Lähikuva – Audiovisuaalisen Kulttuurin Tieteellinen Julkaisu, 32 (3), 26–45
Warr, P. and Parker, S. (2010), IWP multi-affect indicator, (Unpublished instrument), Sheffield, UK: Institute of Work Psychology, University of Sheffield.
Affect: A construct (e.g., psychological) that varies along continuums in three dimensions: Arousal, Valence and Motivation.
Autonomous Sensory Meridian Response (ASMR): A “tingling” sensory-perceptual experience in response to audio-visual or haptic stimuli.
Bonferroni correction: A multiple comparison correction that is used when several dependent or independent statistical tests are performed simultaneously
Correlation: A statistic measuring the degree to which two variables move in relation to one another.
Statistical significance: A statistical method examining the null hypothesis in which it is hypothesised that the results are due to chance alone.
Thematic Analysis (TA): A flexible data analysis approach for identifying ‘themes’ in the qualitative data set.
To cite this paper please use the following details: Lindfors et al.(2021), 'From Cathartic ‘Brain Tingles’ to Scratching Chalkboard Sensations: An Exploratory Study Investigating the Phenomenological Aspects of ASMR', Reinvention: an International Journal of Undergraduate Research, Volume 14, Issue 2, https://reinventionjournal.org/article/view/743. Date accessed [insert date]. If you cite this article or use it in any teaching or other related activities please let us know by e-mailing us at Reinventionjournal@warwick.ac.uk.