Cody W. Ritz, Brigham Young University, Provo, USA
A review of various approaches to voice feminisation for transgender women reveals two conflicting philosophies concerning voice and gender identity: determinism and constructivism. While the determinist philosophy equates sex with gender and posits that physiology determines vocal output, the constructivist philosophy views gender and vocal differences as more dependent on socio-cultural factors. Much of past research has relied on the deterministic perspective to define the voice as a set of masculine or feminine acoustic measures. This binary categorisation poses a challenge for adult transgender women who must overcome significant laryngeal changes attributed to puberty to modify their voices. Certain studies indicate voice feminisation interventions are more effective when they incorporate the self-perceived identities of transgender women into treatment strategies instead of relying solely on acoustic voice measures to label a voice as either masculine or feminine. Further research suggests that social factors – including class, ethnicity and upbringing – impact vocalisation. In light of this evidence, this paper acknowledges the need for more holistic treatments of the voice through a better integration of the constructivist perspective into voice feminisation practices. In certain reports of patient outcomes, transgender women who rate their voice as more feminine are also perceived as such by listeners. This finding demonstrates the efficacy of a patient-centred approach, which is best accomplished through a synergistic application of both determinist and constructivist philosophies to voice modification. By doing so, therapeutic interventions will likely be more effective at alleviating incongruences between the voice and self-identity for transgender women.
Keywords: Transgender voice, identity construction, voice alteration, voice feminisation, voice and identity, gender identity
The ability to communicate verbally is a unique quality of humankind. For this reason, a person’s vocal output is an integral component of their own identity formation. However, discrepancies between self-identity and vocal output contribute to the incidence of gender dysphoria, or the ‘distress that may accompany the incongruences between one’s experienced or expressed gender and one’s assigned gender’ (APA, 2013). Therefore, the voice has become a centre of interest in transgender studies, particularly for those attempting a masculine-to-feminine (transfeminine) voice shift who must overcome endocrinological barriers to vocalisation (Hari Kumar et al., 2016: 591; Safer and Tangpricha, 2019: 2453). Generally, two modes of thought exist concerning the connection between the human voice and transgender identity: determinism and constructivism (Zimman, 2018: 1–6). The determinist philosophy equates sex with gender and consequently relies on physiology to characterise an individual’s voice; in contrast, the constructivist philosophy distances itself from the biological perspective by acknowledging socio-cultural influences on both gender and voice (Zimman, 2018: 2–3). While different in their approaches, these two philosophies both attempt to provide large-scale theoretical models for the alignment of voice and self-identity.
It is worth acknowledging that in addition to transgender women, people of other genders exist who may also wish to undergo voice feminisation, such as those who identify as non-binary, genderfluid, genderqueer and so on. While examinations of therapeutic strategies for these identities is of importance, the claims in this paper are primarily based on evidence tied to individuals presumed male at birth (PMAB) who currently identify as transgender women. The purpose of this paper is two-fold: firstly to consider the efficacy of determinist and constructivist philosophies in voice feminisation strategies, and secondly – through an analysis of patient outcomes and empirical data – determine how to better apply these philosophies in clinical practice moving forwards. The effectiveness of these two different philosophies will be based upon a consideration of a treatment’s ability to produce tangible changes to vocal output, alter listener perceptions and improve patient-reported satisfaction. Because difficulties with gender-role identity have been attributed to higher rates of suicide attempts (D’Augelli et al., 2005; Maguen and Shipherd, 2010: 35; Remafedi et al., 1991, 1998; Wichstrom and Hegna, 2003), an examination of these opposing approaches for voice modification is of clinical importance, and employing the right strategies in future clinical settings has the potential to improve the quality of life for members of this particularly vulnerable population.
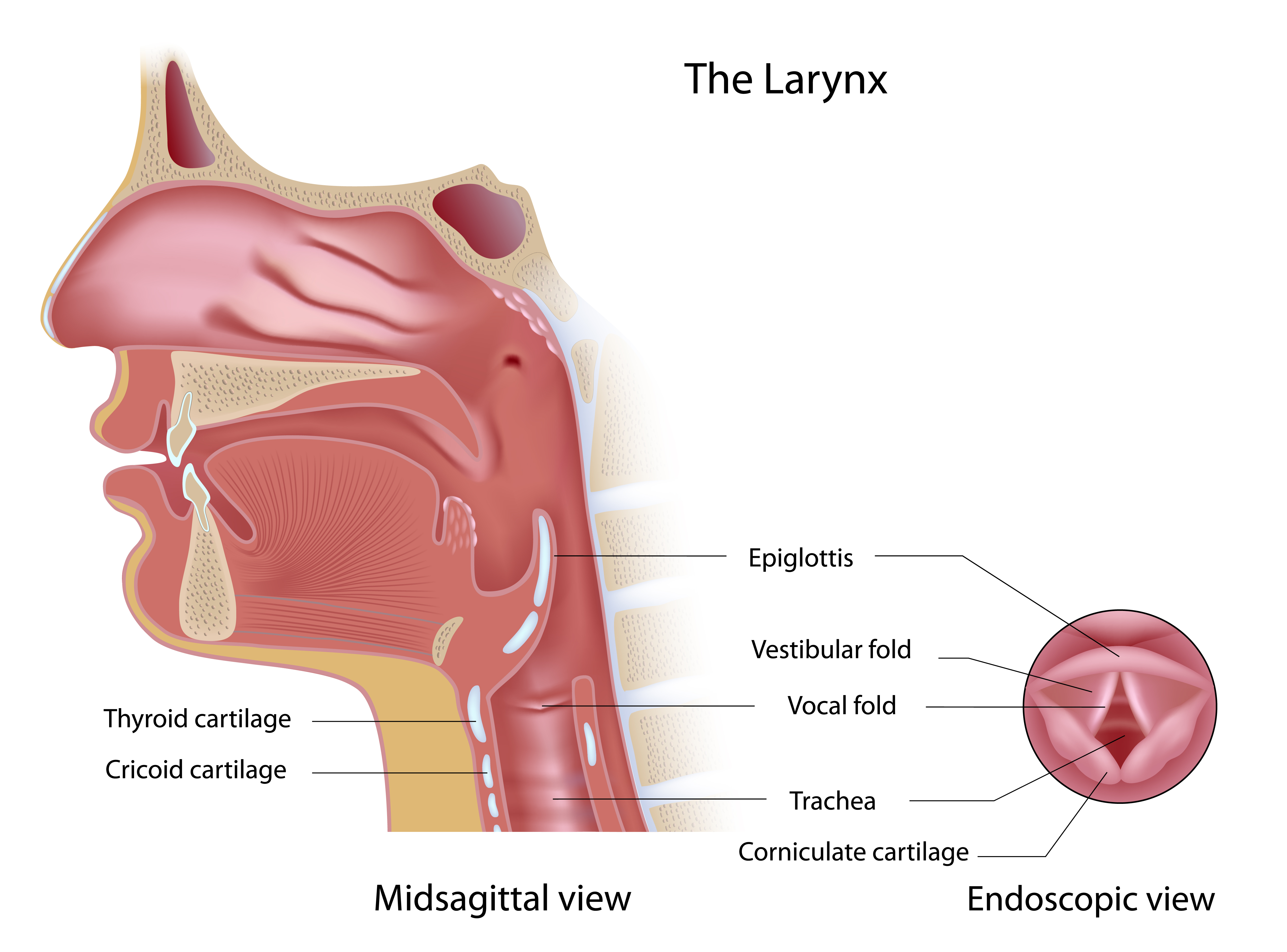
Before exploring the contrast between determinist and constructivist approaches to voice feminisation, it is necessary to understand the underlying physiology of the voice. Vocal output is determined by a complex network of neurological, respiratory and muscular systems working in coordination (Hari Kumar et al., 2016: 590–91). Through this system, the larynx produces sound through vibrations of the vocal folds, and the rate of these vibrations – or fundamental frequency – affects voice pitch, with a higher frequency resulting in a higher-pitched voice (Hari Kumar et al., 2016: 591). However, the larynx is dynamic through its ability to alter its shape and lumen (Hari Kumar et al., 2016: 591). As a result, one person is capable of producing a range of vocal outputs.
Furthermore, pubescent hormones have marked effects on laryngeal shape and structure. Increased testosterone levels in pubescent males thicken the larynx, causing the well-known voice drop that they typically experience (Hari Kumar et al., 2016: 591). In contrast, heightened levels of oestrogen and progestogens in pubescent females have minimal effects on the larynx (Hari Kumar et al., 2016: 591); therefore, testosterone levels seem to be the primary factor in determining vocal differences between the biological sexes.
These physiological differences between the male and female voice present unique challenges for transgender individuals hoping to change the way in which they vocally present themselves. Since the effects of testosterone are not readily reversible, the transfeminine voice transition presents a complicated scenario in which the physiology of the voice must be carefully navigated. While transgender men have access to predominant treatments such as testosterone therapy (Ziegler et al., 2016: 25), transgender women do not have this option, adding an additional layer of difficulty to their therapeutic approaches. For this reason, research into the transfeminine voice transition presents an exciting opportunity to test hypotheses concerning the connections between gender identity and voice (Zimman, 2018: 11).
Because past understandings about the voice have been based primarily on anatomical differences, much of the data regarding the transfeminine voice transition relies heavily on the deterministic perspective. As a result, biological descriptors have become the primary method of classification for differences between masculine and feminine voices (Zimman, 2018: 3). Through this perspective, differences between sex and gender are not readily distinguished. Consequently, researchers who adopt this approach may sometimes rely on their own perceptions and assumptions about the body when classifying the gender identities of participants, even if they do not fully align with a transgender client’s wishes (Zimman, 2018: 3).
One common clinical approach involves exogenous oestrogen therapies to help alter secondary sex characteristics. However, because the effects of testosterone primarily occur during puberty (Hari Kumar et al., 2016: 591), post-pubertal oestrogen therapies are unable to induce significant vocal changes (Quinn and Swain, 2018: 1–2). This reality is increasingly complicated by the fact that a large percentage of individuals experiencing gender incongruence do not report so until late adolescence or adulthood (Rider et al., 2018; Safer and Tangpricha, 2019: 2452), which is a likely explanation for the lower rates of vocal satisfaction after hormone therapy for individuals in this older age range (Oates and Dacakis, 2015; Van Damme et al., 2017).
For those seeking alternatives to oestrogen therapy, a number of clinical options for voice modification still exist through the route of phonosurgery. Vocal fold-shortening procedures, such as anterior glottic web formation and cricothyroid approximation, are available to increase a voice’s fundamental frequency (Van Damme et al., 2017: 244.e1). While phonosurgery can be effective in accomplishing its goal of raising a voice’s pitch, current surgical interventions cannot account for other aspects of the voice such as ‘airflow, resonance or formant ranges, intonation, and intensity’ (Gray and Courey, 2019: 714). Furthermore, these procedures are unable to address non-verbal communication standards that may vary depending on one’s cultural background and environment (Gray and Courey, 2019: 714). Essentially, phonosurgery reduces the voice’s gender identity to its pitch. Therefore, this approach epitomises the determinist assertion that physiology dictates vocal output.
In contrast to phonosurgery, less invasive alternatives are offered through voice therapy. Individuals seeking this route of voice feminisation may also discover a heavy reliance on the determinist perspective since acoustic measures for cis-male and cis-female voices often dictate therapeutic strategies. For example, early literature suggests that average fundamental frequencies must settle around 155 Hz for connected speech (Gelfer and Schofield, 2000; Wolfe et al., 1990) and up to 180 Hz for vowels (Gorham-Rowan and Morris, 2006) in order for a client’s voice to fit inside preconceived boundaries of a feminine voice. Furthermore, cis-female voices have been described to have a ‘breathiness’ that results from friction between vocal folds that do not close completely (Van Borsel et al., 2009: 291). In addition to these factors, other potential sex-distinguishable measures include intonation (Fitzsimons et al., 2001; Owen and Hancock, 2010), intensity (Mészáros et al., 2005), articulation (Mészáros et al., 2005) and inflection (Owen, 2009; Owen and Hancock, 2010). While much of this literature serves to make distinctions concerning voice perception, the data typically stems from a primarily white patient population under traditional Western notions of gender normativity (Stryker, 2014: 15; Zimman, 2018: 2, 7). As a result, these measures have inherent levels of bias, which immediately reveal their shortcomings when trying to apply them more broadly to understand the alignment of voice and gender identity.
While myriad acoustic measures describe the quality of the human voice, most voice therapies have centred on fundamental frequency and resonance. Frequency is altered by vibration speed of the vocal folds, and resonance is the result of ‘rounding or retracting the lips and changing the place and extent that the vocal tract is constricted’ (Hancock and Garabedian, 2013: 55–56). Concentrating on these two factors has been deemed the most effective technique for altering the perceived quality of the voice (Gelfer and Mikos, 2005; Hillenbrand and Clark, 2009). Certain therapeutic interventions are accomplished through systematic exercises that target aspects of laryngeal muscle tension, and through this method, deterministic goals for transfeminine voice transitions have proven to be effective in achieving their primary purpose: raising a voice’s fundamental frequency (Gelfer and Tice, 2013; Gelfer and Van Dong, 2013; Mészáros et al., 2005; Quinn and Swain, 2018: 3). However, there is a need to further explore the clinical significance of this approach since fundamental frequency alone does not account for every factor impacting someone’s voice quality.
Looking at patient outcomes in determinist voice interventions reveals important insight regarding the effectiveness of these clinical approaches for voice feminisation. Focusing solely on increasing fundamental frequency is not sufficient for clients to be consistently perceived as feminine because no consensus exists around a frequency level that can be decisively deemed as feminine in all cases (Dacakis et al., 2012: 165–66). Although interventions may produce higher fundamental frequencies, there is significant individual variation, and some results may not be significant enough for clients to be perceived as feminine by listeners (Oates and Dacakis, 2015; Quinn and Swain, 2018: 11). One can also turn to patient-reported treatment effectiveness and satisfaction for an indication of whether or not clinical approaches are truly improving patient quality of life. Whether voice transition interventions are surgical or therapeutic, there is some indication that long-term maintenance of higher fundamental frequencies can be maintained (Dacakis, 2000: 550–51). However, there is a need for more data regarding the long-term efficacy of these interventions (Dacakis, 2000: 550–51; Gray and Courey, 2019: 715–19). Despite this lack of evidence, short-term data presented through the Trans Woman Voice Questionnaire (TWVQ) – previously known as Transsexual Voice QuestionnaireMtF – also provides some insight into the effectiveness of voice therapy interventions.
The TWVQ essentially measures an individual’s perception of their own voice. This assessment tool also analyses how participants are able to integrate their voice into everyday life, and its reliability has been supported by a high level of consistency across studies (Cardell and Ruda, 2014; Dacakis et al., 2013, 2017: 835–37; Davies and Johnston, 2015; Santos et al., 2015). In one such study, a strong correlation was discovered between the TWVQ scores of 148 transgender women and self-reported perceptions of their voice’s level of femininity (Dacakis et al., 2017: 833–37). In contrast, no such correlation was proven to be significant between TWVQ scores and acoustic voice characteristics such as frequency and voice quality (Dacakis et al., 2017: 835–37). In other words, the self-perception of these transgender women is a more important indicator for the alignment of their voices and identities than deterministic measures that qualify their voices as simply male or female. This evidence provides strong support to the idea that an overemphasis on the acoustic parameters of the voice does not always help clients settle at a voice that fits their gender identity. As a result, this limited deterministic approach is unable to address issues tied to gender dysphoria in every case.
Additional research findings posit that a more holistic perspective must be applied to transfeminine voice transitions. Empirical data demonstrate that clients’ self-perceived vocal femininity is the strongest correlate for voice satisfaction (Quinn and Swain, 2018: 4). This claim illustrates that aligning voice and gender identity involves more than just acoustic measures and suggests that additional factors – such as those considered by the constructivist philosophy – also contribute to one’s overall voice experience (Dacakis et al., 2012: 166–69).
The constructivist perspective offers a potential counterbalance to the physiologically focused determinist point of view. Instead of relying entirely upon anatomy, the constructivist philosophy acknowledges that voice and gender differences are partially – if not entirely – the result of social constructs (Azul and Hancock, 2020: 8–9). Furthermore, constructivism defines the speaker’s ‘vocal behavior’ as an important factor contributing to a person’s vocal identity (Azul and Hancock, 2020: 8–9). Integrating the constructivist mindset of voice and gender identity in clinical practice may overcome limitations imposed by determinism’s binary perspective. An examination of past research and additional patient outcomes related to the constructivist philosophy will evaluate the validity of this approach for voice feminisation practices.
Studies involving the voice of pre-pubertal children provide interesting support for the application of the constructivist perspective to clinical practice. Although considerable differences exist among their fundamental frequencies, children’s vocal tracts do not differ substantially enough on their own to account for such a vast degree of variation; therefore, researchers attribute these differences to the processes of language acquisition and socialisation (Zimman, 2018: 5). This evidence suggests that children may be able to exert even more control over their voices than originally thought. This type of control owes itself to a child’s ability to settle at varying frequencies depending on how they choose to manipulate their voice (Zimman, 2018: 6). Over time, their vocal tracts may end up shorter or longer than they would otherwise be without conscious manipulation (Zimman, 2018: 6), suggesting that socialisation plays a role in the formation of someone’s voice and even has the capacity to affect physiology. This evidence indicates that vocal output is more malleable than traditionally thought. Indeed, the human voice has a variety of ranges that can be attributed to one person; yet the formative processes during one’s youth may determine the range at which this individual’s voice settles. These facts coincide with the sentiments of some in the trans community who have expressed a belief that ‘genital configurations don’t undermine facts about who [they] are’ (Bettcher, 2014: 385–389). To truly adopt this viewpoint into clinical practice, even further emphasis must be placed on aiding transgender women from a young age – or as soon as possible – to ensure that they are in social situations in which they feel comfortable altering their voice to fit their self-perceived identity.
The reported impacts of socialisation on vocal output further suggest the benefits of a constructivist mindset. Stuart-Smith (2007) found that vocal differences combine with socio-economic status among young cisgender women in Glasgow. Specifically, young working-class women produced a lower frequency /s/ more similar to that of cisgender men; meanwhile, middle-class women aligned more closely with the general population of cisgender women (Stuart-Smith, 2007). Additionally, ethnicity has its own connection to the voice. For instance, Japanese-speaking cisgender women have been shown to have higher fundamental frequencies on average than their American English-speaking counterparts, and the opposite is true when comparing Japanese and American cisgender men (Loveday, 1981; Yuasa, 2008). In another study that examined seven primarily indigenous languages, only one of these languages (Chickasaw) demonstrated significant differences between male and female /s/ frequencies (Gordon et al., 2002). These findings demonstrate the socio-cultural influences on the human voice. By being encouraged to see this perspective, those wishing to undergo voice feminisation may feel more comfortable in understanding that their vocal output is determined by a litany of factors. As a result, transgender women may be more at ease even if they cannot fully pass into a more feminine vocal range as defined by a set of one-dimensional physiological parameters.
Client comments regarding the voice modification goals promoted in the Pacific University Transgender Voice Program provide some insight into the usefulness of constructivism in clinical practice. This programme employs approaches that target fundamental frequency and resonance, with clients choosing for themselves whether or not to aim for a passing grade. In R. Bourland’s video posted by Pacific University (2019), Lana Zeitler – one of the programme’s clients – reveals that there is some debate in the trans community about the importance of passing. She expresses her contentment with ‘being in the middle’ because it frees her from the added pressure of feeling as if she must absolutely pass the test in order to reform her identity. Her opinion echoes the sentiments of some transgender scholars, such as Sandy Stone, who criticise the concept of passing because it inherently suggests that transgender individuals must present themselves as either masculine or feminine and not anything between (1991: 294–96). This perspective clearly outlines the importance of gender malleability. Based on Zeitler’s words and the reported results of the TWVQ mentioned earlier in this paper, a heavy-handed focus on the voice’s acoustic components fails to provide a malleable framework for vocal identity that is capable of accommodating greater diversity in gender identities, and consequently, fewer patients experience satisfaction with their treatments. For this reason, the constructivist approach could prove to be beneficial in voice feminisation therapies because it acknowledges more flexibility to one’s vocal output, allowing for a multiplicity of frequency ranges aligning with various identities.
There are some studies that recognise growing support for the utility of constructivism in clinical practice. In an article posted in the International Journal of Transgenderism, Davies et al. (2015) advocate that speech-language therapists must be sensitive to the client’s wishes instead of following overreaching assumptions about a person’s goals related to voice and communication. They also claim that understanding the client’s own perception of the voice is useful in determining the effectiveness of voice therapy (Davies et al., 2015: 119). Because transgender women who rate their vocal behaviour as more feminine are also perceived as such by listeners (Davies et al., 2015: 122), speaker perceptions – as opposed to that of listeners – should be a top priority for voice feminisation approaches. Many transgender women even feel less pressure to feminise their voice after gender reassignment surgery, suggesting that the need to sound more feminine may be less important if other incongruences between the body and gender identity can be remedied in some way (Davies et al., 2015: 121). Although a single-minded emphasis on physiology has proven to be less effective, this evidence suggests that physiologically focused interventions can still prove useful and should not be ignored. Indeed, determinist and constructivist mindsets may work in harmony if each is given credence depending on the needs of the client. This harmonious approach is what Azul and Hancock refer to as the ‘biocultural assemblage view’ of the voice, which they regard as the most ‘comprehensive theoretical perspective’ (2020: 9). Through this point of view, an overemphasis on either constructivism or determinism is inadequate; instead, it is the combined understanding of both the physiological underpinnings and intersectionality of the human voice that has perhaps the greatest potential to facilitate client satisfaction. If transgender women understand that vocal femininity is tied to sociocultural factors in addition to anatomy, then they will be more empowered to find a voice that truly fits their identity.
The voice is one of many components contributing to someone’s gender identity, and within the voice itself are a number of physiological and socio-cultural influences determining vocal output. Evaluating the ability of various treatments to produce tangible changes to vocal output, alter listener perceptions and improve patient-reported satisfaction has demonstrated that a singular focus on physiological factors does not fully address the complex task of voice feminisation for transgender women. However, a complete exclusion of anatomical factors also appears to be inadequate. Therefore, constructivism must be incorporated alongside determinism in clinical practice to comprehensively treat clients according to their needs. Given society’s ever-evolving understanding of the relationship between sex and gender, we lack a general consensus concerning the best practical approaches to solve issues related to gender dysphoria. However, it is important to understand that ‘practice…precedes evidence’ (Davies et al., 2015: 119); therefore, research must continually integrate the constructivist philosophy into voice feminisation approaches that may have previously been only deterministically focused. Employing both of these approaches in a synergistic manner may help a much wider array of transgender women arrive at their desired vocal outcomes and offer greater relief to feelings of gender dysphoria. While this paper has primarily focused on voice feminisation for transgender women, future studies must invest in better understanding voice interventions for those of other gender identities such as transgender men, non-binary, genderfluid, genderqueer and so on. Additionally, further research must extend beyond the scope of a traditionally white Western perspective of vocal identity in order to gain a broader understanding of the ‘complex interplay between race, ethnicity and transgender phenomena’ (Stryker, 2014: 15). Expanding our understanding of voice identification across varying ethnic groups could yield useful information concerning the broader connections between the alignment of one’s voice and gender identity.
I express immense gratitude to my professor, Dr Francesca Lawson, for her valuable support and assistance throughout this project.
Figure 1: Illustration of basic laryngeal structures. Image produced by Alila Medical Media but licensed and obtained through Shutterstock.
American Psychiatric Association (2013), Diagnostic and Statistical Manual of Mental Disorders V, Arlington: American Psychiatric Publishing (originally published in 1952)
Azul, D. and A. B. Hancock (2020), ‘Who or what has the capacity to influence voice production? Development of a transdisciplinary theoretical approach to clinical practice addressing voice and the communication of speaker socio-cultural positioning’, International Journal of Speech-Language Pathology, 1–12 https://doi.org/10.1080/17549507.2019.1709544
Bettcher, T. M. (2014), ‘Trapped in the wrong theory: Rethinking trans oppression and resistance’, Signs, 39 (2), 383–406 https://doi.org/10.1086/673088
Bourland, R. (2019), ‘Pacific University Transgender Program’, available at https://youtu.be/z3_kvPR1Uzc, accessed 13 February 2020
Cardell, F. and M. Ruda (2014), ‘Reliability evaluation of the Swedish version of Transsexual Voice QuestionnaireMale-to-Female (TVQMtF)’, unpublished master’s thesis, Karolinska Institute
D’Augelli, A. R., A. H. Grossman, N. P. Salter, J. J. Vasey, M. T. Starks and K. O. Sinclair (2005), ‘Predicting the suicide attempts of lesbian, gay, and bisexual youth’, Suicide and Life Threatening Behavior, 35 (6), 646–60
Dacakis, G. (2000), ‘Long-term maintenance of fundamental frequency increases in male-to female transsexuals’, Journal of Voice, 14 (4), 549–56
Dacakis, G., S. Davies, J. Oates, J. M. Douglas and J. R. Johnston (2013), ‘Development and preliminary evaluation of the Transsexual Voice Questionnaire for male-to-female transsexuals’, Journal of Voice, 27 (3), 312–20
Dacakis, G., J. Oates and J. Douglas (2012), ‘Beyond voice: perceptions of gender in male-to-female transsexuals’, Current Opinion in Otolaryngology & Head and Neck Surgery, 20 (3), 165–70 https://doi.org/10.1097/MOO.0b013e3283530f85
Dacakis, G., J Oates and J. Douglas (2017), ‘Associations between the Transsexual Voice Questionnaire (TVQMtF) and self-report of voice femininity and acoustic voice measures’, International Journal of Language & Communication Disorders, 52 (6), 831–38 https://doi.org/10.1111/1460-6984.12319
Davies, S. and J. R. Johnston (2015), ‘Exploring the validity of the Transsexual Voice Questionnaire for male-to-female transsexuals’, Canadian Journal of Speech-Language Pathology and Audiology, 39 (1), 40–51
Davies, S., V. G. Papp and C. Antoni (2015), ‘Voice and communication change for gender nonconforming individuals: Giving voice to the person inside’, International Journal of Transgenderism, 16 (3), 117–59 https://doi.org/10.1080/15532739.2015.1075931
Fitzsimons, M., N. Sheahan and H. Staunton (2001), ‘Gender and the integration of acoustic dimensions of prosody: Implications for clinical studies’, Brain and Language, 78 (1), pp. 94–108
Gelfer, M. P. and V. A. Mikos (2005), ‘The relative contributions of speaking fundamental frequencies to gender identification based on isolated vowels’, Journal of Voice, 19, 544–54
Gelfer, M. P. and K. J. Schofield (2000), ‘Comparison of acoustic and perceptual measures of voice in MtF transsexuals perceived as female versus those perceived as males’, Journal of Voice, 14 (1), 22–33
Gelfer, M. P. and R. M. Tice (2013), ‘Perceptual and acoustic outcomes of voice therapy for male-to-female transgender individuals immediately after therapy and 15 months later’, Journal of Voice, 27 (3), 335–347
Gelfer, M. P. and B. R. Van Dong (2013), ‘A preliminary study on the use of vocal function exercises to improve voice in male-to-female transgender clients’, Journal of Voice, 27 (3), 321–34 http://dx.doi.org/10.1016/j.jvoice.2012.07.008
Gordon, M., P. Barthmaier and K. Sands (2002), ‘A cross-linguistic acoustic study of voiceless fricatives’, Journal of the International Phonetic Association, 32 (2), 141–74 https:// doi.org/10.1017/S0025100302001020
Gorham-Rowan, M. and R. Morris (2006), ‘Aerodynamic analysis of male-to-female transgender voice’, Journal of Voice, 20 (2), 251–62
Gray, M. L. and M. S. Courey (2019), ‘Transgender voice and communication’, Otolaryngologic Clinics of North America, 52 (4), 713–22
Hancock, A. B. and L. M. Garabedian (2013), ‘Transgender voice and communication treatment: A retrospective chart review of 25 cases’, International Journal of Language & Communication Disorders, 48 (1), 54–65 https://doi.org/10.1111/j.1460-6984.2012.00185.x
Hari Kumar, K. V. S., A. Garg, N. S. Ajai Chandra, S. P. Singh and R. Datta (2016), ‘Voice and endocrinology’, Indian Journal of Endocrinology and Metabolism, 20 (5), 590–94 https://doi.org/10.4103/2230-8210.190523
Hillenbrand, J. M. and M. J. Clark (2009), ‘The role of fundamental frequency and formant frequencies in distinguishing the voices of men and women’, Attention, Perception, and Psychophysics, 71(5), 1150–66
Loveday, L. (1981), ‘Pitch, politeness and sexual role: An exploratory investigation into the pitch correlates of English and Japanese politeness formulae’, Language and Speech, 24 (1), 71–88. https://doi.org/10.1177/002383098102400105
Maguen, S. and J. C. Shipherd (2010), ‘Suicide risk among transgender individuals’, Psychology & Sexuality, 1 (1), 34–43 https:/doi.org10.1080/19419891003634430
Mészáros K, L. C. Vitéz, I. Szabolcs, M. Góth, L. Kovács, Z. Görömbei and T. Hacki (2005), ‘Efficacy of conservative voice treatment in male-to-female transsexuals’, Folia Phoniatrica et Logopaedica, 57(2), 111–18
Oates, J. and G. Dacakis (2015), ‘Transgender voice and communcation: Research evidence underpinning voice intervention for male-to-female transsexual women’, Perspectives on Voice and Voice Disorders, 25 (2), 28–58
Owen, K. (2009), ‘Comparing self-perceptions to subjective and objective measures of femininity in transgender speakers’, unpublished master’s thesis, George Washington University
Owen, K. and A. B. Hancock (2010), ‘The role of self- and listener perceptions of femininity in voice therapy’, International Journal of Transgenderism, 12 (4), 272–84
Quinn, S., and N. Swain (2018), ‘Efficacy of intensive voice feminisation therapy in a transgender young offender’, Journal of Communication Disorders, 72, 1–15 https://doi.org/10.1016/j.jcomdis.2018.02.001
Remafedi, G., J. A. Farrow and R. W. Deisher (1991), ‘Risk factors for attempted suicide in gay and bisexual youth’, Pediatrics, 87 (6), 869–75
Remafedi, G., S. French, C. Story, M. D. Resnick and R. Blum (1998), ‘The relationship between suicide risk and sexual orientation: Results of a population-based study’, American Journal of Public Health, 88 (1), 57–60
Rider, G. N., B. J. McMorris, A. L. Gower, E. Coleman and M. E. Eisenberg (2018), ‘Health and care utilization of transgender and gender non-conforming youth: A population-based study’, Pediatrics, 141 (3), e20171683 https://doi.org/10.1542/peds.2017-1683
Safer, J. D. and V. Tangpricha (2019), ‘Care of transgender persons’, New England Journal of Medicine, 381 (25), 2451–60 https://doi.org/10.1056/NEJMcp1903650
Santos, H., H. Aguiar, A. G, H. E. Baeck and J. Van Borsel (2015), ‘Translation and preliminary evaluation of the Brazilian Portuguese version of the Transgender Voice Questionnaire for male‐to‐female transsexuals’, Communication Disorders and Sciences, 27 (1), 89–96
Stone, S. (1991), ‘The ‘Empire’ Strikes Back: A posttranssexual manifesto’, in Epstein, J. and K. Straub (eds), Body Guards: The cultural politics of gender ambiguity, New York: Routledge, pp. 280–304
Stryker, S. (2014), ‘(De)subjugated knowledges: an introduction to transgender studies’, in Stryker, S. and S. Whittle (eds), The Transgender Studies Reader, New York: Routledge Taylor and Francis Group, pp. 1–17
Stuart-Smith, J. (2007), ‘Empirical evidence for gendered speech production: /s/ in Glaswegian’, in Cole, J. and J. I. Hualde (eds), Laboratory Phonology 9, 65–86
Van Borsel, J., J. Janssens, and M. De Bodt (2009), ‘Breathiness as a feminine voice characteristic: A perceptual approach’, Journal of Voice, 23 (3), 291–94
Van Damme, S., M. Cosyns, S. Deman, Z. Van den Eede and J. Van Borsel (2017), ‘The effectiveness of pitch-raising surgery in male-to-female transsexuals: A systematic review’, Journal of Voice, 31 (2), 244.e1-244.e5 https://doi.org/10.1016/j.jvoice.2016.04.002
Wichstrom, L. and K. Hegna (2003), ‘Sexual orientation and suicide attempt: A longitudinal study of the general Norwegian adolescent population’, Journal of Abnormal Psychology, 112 (1), 144–51
Wolfe, V. I., D. L. Ratusnik, F. H. Smith and G. Northrop (1990), ‘Intonation and fundamental frequency in male-to-female transsexuals’, Journal of Speech and Hearing Disorders, 55 (1), 43–50
Yuasa, I. P. (2008), ‘Culture and gender of voice pitch: A sociophonetic comparison of the Japanese and Americans’, Language in Society, 40 (2), 251–52
Ziegler, A., T. Henke, J. Wiedrick and L. B. Helou (2018), ‘Effectiveness of testosterone therapy for masculinizing voice in transgender patients: A meta-analytic review’, International Journal of Transgenderism, 19 (1), 25–45 https:doi.org10.1080/15532739.2017.1411857
Zimman, L. (2018), ‘Transgender voices: Insights on identity, embodiment, and the gender of the voice’, Language and Linguistics Compass, 12 (8), 1–16 https://doi.org/10.1111/lnc3.12284
Anterior glottic web formation: Formation of new tissue that narrows portions of the larynx; can raise vocal pitch.
Articulation: The action of placing certain emphases on consonant sounds while speaking.
Cricothyroid approximation: Procedure in which laryngeal muscle tension is altered to raise vocal pitch.
Gender*: Identity within the context of social roles; formed on an individual basis and developed over the course of one’s life; independent of biology.
Inflection: changes to pitch or intensity while speaking that imply additional meaning to words or phrases.
Intensity: The loudness of a person’s voice while speaking.
Intonation: The variation and combination of vocal tones utilised while speaking.
Lumen: The interior cavity of a tube-like anatomical organ or structure; often utilised for the exchange of liquid, gases and nutrients.
Phonosurgery: Surgical interventions that focus specifically on changes to anatomical structures to impact someone’s vocal output. The interior cavity of a tube-like anatomical organ or structure; often utilised for the exchange of liquid, gases and nutrients.
Sex*: Identity within a biological context; based on physiological factors
To cite this paper please use the following details: Ritz, C.W. (2020), 'Constructivism and Determinism: An examination of two conflicting philosophies to voice feminisation for transgender women', Reinvention: an International Journal of Undergraduate Research, Volume 13, Issue 2, https://reinventionjournal.org/article/view/640. Date accessed [insert date]. If you cite this article or use it in any teaching or other related activities please let us know by e-mailing us at Reinventionjournal@warwick.ac.uk.